




Snapping Hip Syndrome
Snapping hip or “coxa saltans” is a clinical condition characterized by an audible or palpable snap of the
hip. It is a common pathology, and it is frequently asymptomatic. In few cases the snap is painful, and this condition is known as Snapping Hip Syndrome (SHS). Snapping hip is a common condition, it is usually asymptomatic, but when the snap becomes painful and does not respond to conservative treatment, surgery is indicated.
Signs and symptoms:
- Snapping or popping in the front, side, or back of the hip when lifting, lowering, rotating, or swinging the leg
- Weakness in the leg when trying to lift it forward or sideways
- Tightness in the front, back, or side of the hip
- Swelling in the front, back, or side of the hip
- Difficulty performing daily activities, such as rising from a chair and walking.
There are two types of SHS :
- External or lateral snapping hip syndrome (ESHS).
- Internal or medial snapping hip syndrome (ISHS).
Causes of snapping hip syndrome :
1. External or lateral snapping hip syndrome (ESHS):
It is caused by the iliotibial band slides over the greater trochanter, and it may be enhanced by a thickening of the anterior border of the gluteus maximus or of the posterior part of the iliotibial tract.
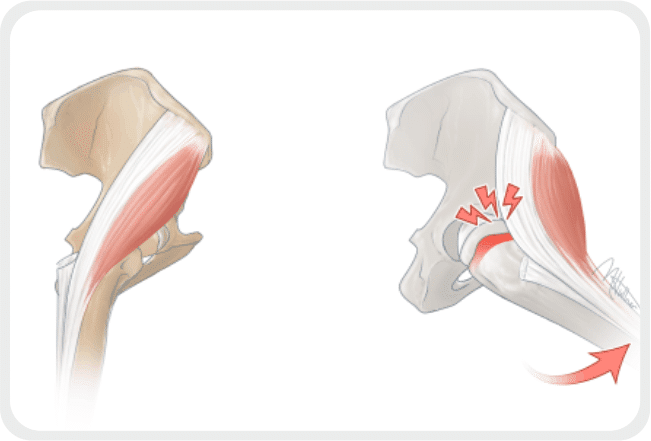
2. Internal or medial snapping hip syndrome (ISHS):
ISHS is commonly believed to be caused by the iliopsoas tendon snapping over the anterior femoral head or the iliopectineal eminence.
3. Conservative treatment for ESHS:
It is important to identify the source of the muscle tightness that is responsible for the snap. Passive and active stretching is effective in most cases to reduce the tightness of the ITB and to solve the snap. However, sometimes the thigh ITB is due to excessive muscle activation which increases muscle tension. In these cases, the intervention is directed to modify neuromuscular control and neuromuscular re-education is indicated. Нence, it is important to solve the imbalance between gluteus maximus activation and tensor fasciae latae activation which is often observed. It is important to not exacerbate symptoms during physical therapy. Good results have been reported after 6 to 12 months of physical therapy, with the resolution of the snap-in most of the patients. To prevent recurrences, modification of lifestyle and stretching exercises are advocated. A precise evaluation of leg lengths is mandatory and, in case of a real discrepancy, equalization with a shoe raise may be used to accompany the physical therapy period.
4. Conservative treatment for ISHS:
Conservative management of ISHS is focused on iliopsoas tendon stretching and muscular balance. As a high iliopsoas muscle activation and a weakness of gluteus medius have been found in many patients, a rehabilitative protocol is based on gluteus medius strengthening.
